Breast Microcalcifications: What They Mean and When They Require Evaluation
The Microcalcifications are small calcium deposits within the breast tissue that are detected exclusively through mammography. They appear as small white spots, mainly in women over 50 years of age, and do not cause symptoms. They are a common mammographic finding, which in most cases is benign, but in some cases may indicate precancerous lesions or even early breast cancer.
What causes microcalcifications?
The appearance of calcifications in the breast can be associated with multiple factors, such as:
- Age (especially postmenopausal)
- Inflammation or trauma to the breast
- Benign entities (fibroadenoma, cysts, sclerosing adenosis)
- Previous radiation therapy
- Breast cancer
Dietary calcium intake is not linked to the development of calcifications.
Additionally, products like deodorants can leave residues on the skin, creating false calcification images. Therefore, they should be avoided on the day of mammography.
Macrocalcifications vs. Microcalcifications
The macrocalcifications are larger, benign, and do not require further investigation. In contrast, the Microcalcifications They are microscopic (they look like grains of sugar on a mammogram) and require attention when they present characteristics associated with malignancy.
When are microcalcifications considered suspicious?
According to the criteria of ACR BI-RADS®, Microcalcifications are considered suspicious when they show:
- Clustering or grouping
- Asymmetry between breasts
- Linear or branching distribution
- Variability in size and morphology
In such cases, it is requested magnification mammography for a better assessment and, depending on the findings, may be recommended:
- Follow-up in 6 months
- Biopsy
- Return to annual screening
Microcalcifications as an early sign of cancer
When microcalcifications are associated with malignancy, the most common possibility is that they indicate ductal carcinoma in situ (DCIS) — a non-invasive precancerous lesion, with an extremely good prognosis and a probability of metastasis of <1%.
Detection of microcalcifications by mammography is often the only way to diagnose DCIS, as it does not cause palpable masses or symptoms in early stages.
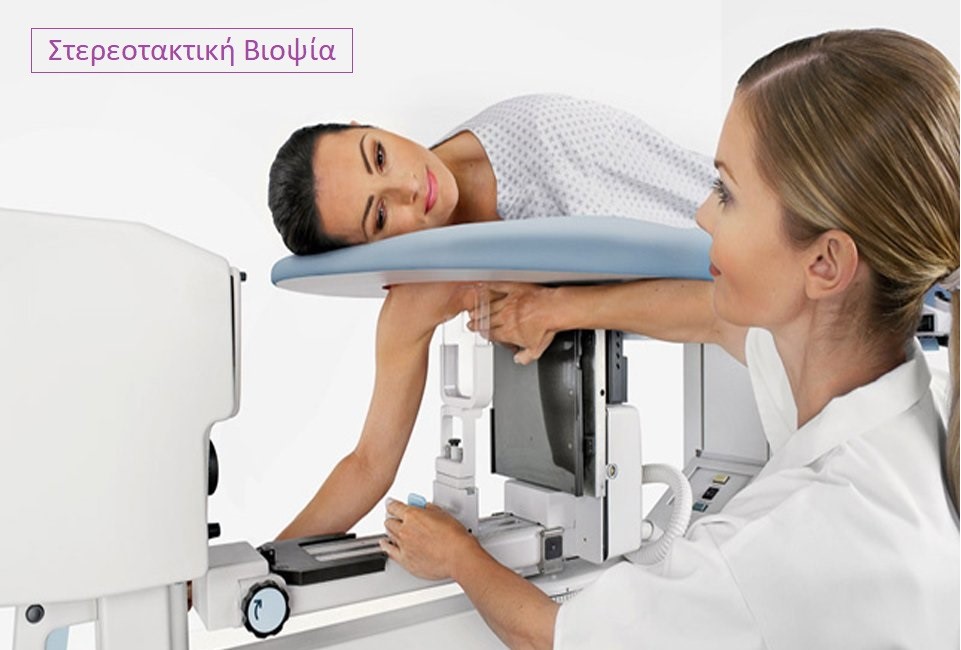
How is the biopsy of microcalcifications performed?
Biopsy of suspected microcalcifications is mainly performed using the method of stereotactic biopsy. This is a targeted process that includes:
- Local anesthesia
- Computed guidance based on mammographic coordinates
- Sample collection with a specialized cutting needle
Stereotactic biopsy is the preferred method for sampling calcifications detected solely by mammography, following international guidelines (NCCN, ACR).
When stereotactic biopsy is not possible, it is performed surgical biopsy guided by a guide wire, which is placed preoperatively based on mammographic coordinates.
What happens after the biopsy?
The final diagnosis is determined by the pathological examination. Depending on the findings, it may follow:
- Surveillance
- Additional surgical intervention
- Systemic therapy
The preventive mammography proves to be a crucial tool for the early diagnosis breast cancer in early stages.
breastaware.gr – Knowledge is Prevention
At breastaware.gr you will find reliable and scientifically supported information on breast prevention, diagnosis, and care. Get informed and make prevention part of your life.
Bibliography:
- Berg WA, et al. ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System. 5th ed. Reston, VA: American College of Radiology; 2013.
- Lehman CD, et al.. Diagnostic accuracy of digital screening mammography with and without computer-aided detection. JAMA Intern Med. 2015;175(11):1828–1837.
- O'Grady KF, et al.. Breast microcalcifications: Pathological significance and diagnostic implications. Clin Radiol. 2020;75(5):360–366.
- Liberman L, Menell JH. Breast imaging reporting and data system (BI-RADS). Radiol Clin North Am. 2002;40(3):409–430.
- Elmore JG, et al. Variability in pathologists' interpretations of individual breast biopsy slides: a population perspective. Ann Intern Med. 2015;162(2):85–91.
- Holland R, Hendriks JH, Mravunac M. Mammographically occult ductal carcinoma in situ (DCIS) of the breast. Pathol Annu. 1994;29(Pt 2):177–202.
- D’Orsi CJ. ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System. 5th ed. Reston, VA: American College of Radiology; 2013.
- Jochelson MS. Imaging issues in screening women at high risk for breast cancer. Breast J. 2020;26(6):1241–1248.
- Ghai S, et al.. Microcalcifications: a multimodality approach to diagnosis and management. Insights Imaging. 2020;11(1):119.
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology: Breast Cancer. Version 4.2025. Available at: